


宫颈高级别鳞状上皮内病变(HSIL)是宫颈癌的前驱病变,除非治疗得当,否则可能进展为宫颈癌[1]。HSIL病变的推荐治疗方法是锥切术,然后进行常规的人乳头瘤病毒(HPV)和(或)宫颈细胞学检查[2]。宫颈锥切术后复发危险因素包括切缘阳性、高危型HPV感染、腺体受累及年龄等[3⇓⇓-6]。其中切缘阳性是最重要的复发危险因素,无生育要求者可以考虑再次手术治疗[7]。与切缘阳性不同,对腺体受累及HPV持续感染患者临床处理存在争议,该2项因素在HSIL中的临床意义尚未得到广泛认可,结合腺体受累及HPV感染分析其对HSIL复发的影响鲜有报道。本研究根据宫颈腺体受累和HPV感染情况对接受宫颈冷刀锥切术治疗的HSIL患者进行了临床预后研究,评估两者对HSIL患者临床病程的影响。
对象与方法
一、研究对象
2016年1月至2020年6月在唐山市工人医院及唐山市妇幼保健院行宫颈冷刀锥切术治疗的HSIL患者共596例,其中腺体受累240例、腺体未受累356例。本研究为回顾性研究,样本量功效大于80%,样本量可保证研究结论具有一定可靠性。纳入标准:①经组织病理诊断为HSIL;②术后每6个月复查HPV和(或)进行宫颈脱落细胞检测;③可获取患者完整的临床病理资料及随访资料。排除标准:①曾行其他宫颈手术治疗;②哺乳期及妊娠期女性;③合并其他恶性肿瘤;④切缘阳性者。本研究已通过唐山市工人医院伦理委员会审查(伦理批件号:GRYY-LL-2019-27)。
二、研究方法
宫颈HPV筛查采用美国罗氏公司的Cobas 4800检测平台进行检测,本检测方法共检测14种高危型HPV(包括HPV-16、HPV-18、HPV-26、HPV-31、HPV-33、HPV-35、HPV-39、HPV-45、HPV-52、HPV-56、HPV-58、HPV-59、HPV-66、HPV-68),并对HPV-16和HPV-18单独分型检测,所有操作均严格按照厂家说明书进行。宫颈冷刀锥切术用卢戈氏碘液显示碘不着色区,沿不着色区域外缘3~5 mm进行切除,锥高切除范围1.5~2.5 cm。宫颈组织病理诊断由一名医师初诊,然后再由一名副主任医师复诊,诊断标准参考2020年第5版子宫颈肿瘤WHO分类。
三、研究流程
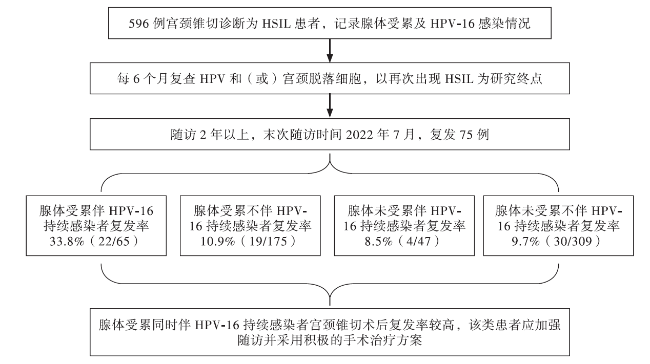
596例患者术前均进行HPV检测,宫颈冷刀锥切术后病理诊断为HSIL,每6个月复查HPV和(或)进行宫颈脱落细胞检测,以随访2年或再次出现HSIL为研究终点,末次随访时间为2022年7月。腺体受累被定义为宫颈腺体结构中出现HSIL,同种型别HPV感染1年及以上判定为持续感染,术后6个月以上再次出现HSIL判定为复发。分析腺体受累和HPV感染对复发的影响。
四、统计学处理
采用SPSS 26.0处理数据。计数资料以例(%)表示,组间比较采用χ2检验。2组间比较P < 0.05为差异有统计学意义。本研究主要关注腺体受累伴HPV-16持续感染患者与腺体受累不伴HPV-16持续感染患者、腺体不受累伴HPV-16持续感染患者和腺体不受累不伴HPV-16持续感染患者间的复发率间差异,故对腺体受累伴HPV-16持续感染组与其他3组间的复发率比较采用Bonferroni法校正,即P < 0.05/3 = 0.017为差异有统计学意义。
结果
一、临床病理资料
HPV-16阳性245例,其中112例为HPV-16持续感染;HPV-18阳性63例,其中HPV-18型持续感染9例;HPV其他12型阳性248例,其中HPV其他12型持续感染35例;HPV阴性40例。随访结束时,复发75例、未复发521例。
二、腺体受累组与腺体未受累组患者的不同型别HPV初次感染情况比较
腺体受累组患者的HPV-16感染率高于腺体未受累组(P < 0.05),HPV-18型及其他12型感染率在腺体受累组与腺体未受累组间比较差异无统计学意义(P均> 0.05)。见表1。
表1 腺体受累组与腺体未受累组患者的不同型别HPV初次感染情况比较[例(%)] |
| 组 别 | 例数 | HPV-16 | HPV-18 | HPV其他12型 |
|---|---|---|---|---|
| 腺体受累组 | 240 | 163(67.9) | 30(12.5) | 102(42.5) |
| 腺体未受累组 | 356 | 82(23.0) | 33(9.3) | 146(41.0) |
| χ2值 | 119.288 | 1.582 | 0.131 | |
| P值 | <0.001 | 0.208 | 0.718 |
三、复发组与未复发组患者的年龄、腺体受累率、HPV-16持续感染情况比较
复发组与未复发组患者的 ≥ 45岁者比例、腺体受累率、HPV-16持续感染率比较差异均无统计学意义(P均> 0.05)。见表2。
表2 复发组与未复发组患者的年龄、腺体受累、HPV持续感染率比较 [例(%)] |
| 组 别 | 例数 | 年龄≥45岁 | 腺体受累 | HPV-16持续感染 |
|---|---|---|---|---|
| 复发组 | 75 | 41(54.7) | 36(48.0) | 20(26.7) |
| 未复发组 | 521 | 233(44.7) | 204(39.2) | 92(17.7) |
| χ2值 | 2.611 | 2.132 | 3.486 | |
| P值 | 0.106 | 0.144 | 0.062 |
四、腺体受累联合HPV-16持续感染对宫颈锥切术后复发的影响
{kind=link}
{kind=link}
讨论
宫颈癌在我国的发病率和病死率居高不下, 2020年我国宫颈癌死亡病例5.3万,占全世界的15.5%,宫颈癌新增病例11万,占全世界的18.2%[8]。降低宫颈癌的患病率和病死率的其中一种有效方法是早期检测和治疗HSIL。HSIL是一种癌前病变,在癌前病变期间给予适当的治疗可有效预防宫颈癌的发生。宫颈锥形切除术是诊断和治疗HSIL的最佳方法。影响HSIL宫颈锥切术后复发的因素众多,包括切缘阳性、腺体受累、高危型HPV感染及患者年龄等[3⇓⇓-6]。其中切缘阳性对复发影响的研究结果较为一致,但有关腺体受累和HPV感染的研究结果不尽相同。本研究选切缘阴性的HSIL患者作为研究对象,重点探讨腺体受累和HPV感染对锥切术后复发的影响。
上述研究仅对腺体受累和HPV感染情况进行单独分析,研究结论存在差异。本研究显示,596例HSIL患者中,HPV-16阳性者最多,而腺体受累患者中的HPV-16感染者比例高于腺体未受累者。虽然复发组与未复发组患者的 ≥ 45岁者比例、腺体受累率、HPV-16持续感染率比较差异均无统计学意义,但进一步对腺体受累和HPV-16持续感染的联合分析显示,腺体受累伴HPV-16持续感染患者的复发率高于其他患者。因此,联合分析腺体受累及HPV-16持续感染情况,对于锥切术后的预后评估及临床处理可能具有重要意义。
综上所述,腺体受累和HPV-16持续感染作为单一因素对HSIL复发的影响尚存在争议,腺体受累与HPV-16感染密切相关,联合分析HSIL患者的腺体受累及HPV-16持续感染情况至关重要,腺体受累同时伴HPV-16持续感染的患者复发率高于其他患者,对于该类患者应考虑采取更积极的随访及治疗方案。