


肺癌是全球发病率和病死率最高的癌症[1-3]。作为非小细胞肺癌的主要类型,近年来肺腺癌的发病率增长迅速,已超过肺鳞癌,约占肺癌病例的40%[4-6]。尽管分子靶向治疗在肺腺癌的治疗中取得了显著进展,但全球范围内该病患者的5年生存率仍不足20%[7-9]。因此,亟须寻找新的高特异度和高灵敏度的生物标志物,以改善肺腺癌的诊断、预后及治疗策略。葡萄糖氨基转移酶3[glucosaminyl(N-acetyl)transferase 3,GCNT3]是一种黏蛋白型合酶,在聚糖合成中发挥重要作用。研究表明,GCNT3在乳腺癌、前列腺癌、结肠癌、胃癌和肝癌等多种癌症中具有关键作用,并与上皮-间质转化(epithelial-mesenchymal transition,EMT)密切相关[10-18]。GCNT3高表达可促进细胞的增殖、迁移和侵袭。然而,GCNT3在肺腺癌中的表达及其对癌细胞生物学行为的影响尚缺乏详细研究。本研究旨在探讨GCNT3基因对肺腺癌细胞增殖、凋亡和侵袭的影响,为肺腺癌的诊断和治疗提供新的潜在生物标志物及分子靶点。
1 材料与方法
1.1 材料
收集2020至2023年在本院行手术治疗的30例肺腺癌患者的癌组织及其对应的癌旁正常组织。纳入标准:经病理活组织检查(活检)确诊为肺腺癌,并有完整的临床和病理资料,癌旁正常组织取自距离肿瘤边缘至少2 cm处,确保样本无肿瘤细胞浸润。排除标准:非原发性肿瘤者,合并其他肿瘤者。30例肺腺癌患者中,男14例、女16例,患者年龄为42~65岁,中位年龄为53岁。所有患者均签署知情同意书,研究方案经医院伦理委员会批准[批件号:(2023)医伦第(018)号]。为避免交叉污染,采样过程严格控制。组织取材后,部分样本经4%多聚甲醛固定以保存组织结构,另一部分样本迅速置于液氮中冷冻保存,并转移至-80 ℃超低温保存。
1.2 主要试剂与仪器
H1650细胞株购自美国模式菌种收集中心,DMEM培养基、胎牛血清、1%青链霉素购自美国Gibco公司,短发夹RNA(short hairpin RNA,ShRNA)慢病毒质粒、TRIzol试剂、SYBR Green试剂盒和Transwell小室购自德国Sigma-Aldrich公司;Lipofectamine 2000转染试剂盒购自美国Invitrogen公司;实时荧光定量PCR(quantitative real-time polymerase chain reaction,RT-qPCR)试剂盒购自日本TaKaRa公司;RT-qPCR引物购自上海生工生物工程有限公司;Annexin V-FITC细胞凋亡检测试剂盒、二喹啉甲酸(bicinchoninic acid,BCA)法试剂盒和细胞计数试剂盒-8(cell counting kit-8,CCK-8)购自上海碧云天生物技术公司。
1.3 细胞培养与转染
将H1650细胞调整至1×104 /mL,每组设3个复孔,置于含10%胎牛血清和1%青链霉素的DMEM培养基中,在37 ℃、5% CO2的条件下进行培养和传代。按照Lipofectamine 2000试剂操作说明,将100 nmol/L的GCNT3 ShRNA(靶序列:5'-GACCCAAAGGTAGATGATAAT-3')转染入H1650细胞,并将细胞暴露于2 mg/L的嘌呤霉素溶液中筛选。转染后的细胞设为Sh GCNT3组,在含1 mg/L嘌呤霉素的培养基中持续培养72 h以维持稳定性。空白对照组即Sh NC组,使用Sh NC通过Lipofectamine 2000转染。
1.4 实时荧光定量PCR法检测GCNT3的mRNA表达水平
每组设3个复孔,使用TRIzol试剂提取样本总RNA,然后依据RT-qPCR试剂盒的操作说明书,将提取的RNA逆转录为cDNA,并以cDNA为模板进行RT-qPCR扩增。GCNT3正向引物:5'-TCTGGGCTGCTATATGCTGC-3',GCNT3反向引物:5'-GTTGATAGACCTCTTTGCTGGAA-3';β-actin正向引物:5'-CATGTACGTTGCTATCCAGGC-3',β-actin反向引物:5'-CTCCTTAATGTCACGCACGAT-3'。产物长度控制为163 bp,β-actin用作内参基因,作为内源性对照。GCNT3基因的相对表达量采用2-ΔΔCt法计算。
1.5 细胞计数试剂盒-8法检测细胞增殖
将Sh NC组与Sh GCNT3组H1650细胞以1×104 /mL接种于96孔培养板中,每组设3个复孔,分别在37 ℃、5% CO2条件下培养24、48、72 h。培养结束后,每孔加入10 µL CCK-8试剂,继续孵育2 h。以磷酸盐缓冲液(phosphate buffer saline,PBS)为空白对照。随后使用酶标仪在450 nm波长下测定各孔的吸光度(A)值。细胞增殖率=(A实验孔-A空白对照孔)/(A对照孔-A空白对照孔)×100%。
1.6 流式细胞仪检测H1650细胞凋亡
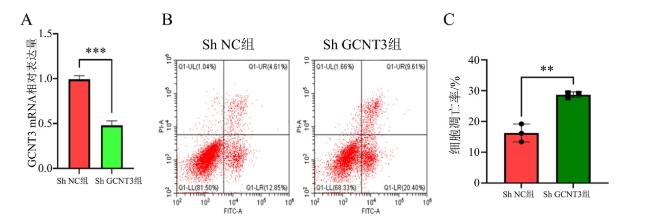
当Sh NC组与Sh GCNT3组H1650细胞融合度达70%~80%时,使用胰蛋白酶消化并用PBS洗涤,制备相应的细胞悬液。每份细胞悬液中加入5 µL Annexin V-FITC试剂,在避光条件下孵育15 min,然后加入5 µL PI(50 mg/L)染色10 min,并向每管加入400 µL结合缓冲液。最后,使用流式细胞仪进行细胞凋亡分析。凋亡率为早期凋亡细胞和晚期凋亡细胞百分率之和。每组设3个复孔。
1.7 Transwell法检测H1650细胞的侵袭能力
将Sh NC组与Sh GCNT3组H1650细胞调整至1.5×105 cells/mL,将基质胶与DMEM培养基按1∶5的比例在冰上混合制备。然后,使用移液枪将稀释后的基质胶缓慢均匀地铺于Transwell上室。接着,在Transwell上室内加入300 µL细胞悬液,而下室添加500 µL含10% FBS的DMEM培养基。细胞培养48 h后,固定并染色穿过Transwell膜的细胞,在显微镜下进行观察。
1.8 蛋白免疫印迹法检测上皮-间质转化相关蛋白的表达水平
收集各组细胞,使用PBS洗涤2次以去除上清液。随后,使用细胞裂解液裂解细胞并提取总蛋白,用BCA试剂盒进行定量。等量的蛋白质样品通过SDS-PAGE分离,并转移至PVDF膜上。膜上用1%脱脂牛奶封闭1 h,然后用含0.1%吐温-20的PBS洗膜3次,每次10 min,接着将膜与相应的一抗在4 ℃摇床上孵育过夜,再用含0.1%吐温-20的PBS洗膜3次,每次10 min。随后,用结合辣根过氧化物酶的二抗孵育。使用ECL化学发光液进行曝光并拍照,以GAPDH作为内参。蛋白免疫印迹法结果使用ImageJ软件进行定量分析。
1.9 统计学方法
采用GraphPad Prism 8.0进行统计分析和图形数据表示,所有数据以$\bar{x}±s$表示,2组间比较采取Student-t检验。每项实验均重复进行3次,数据符合统计分析的假设。双侧P < 0.05为差异具有统计学意义。
2 结果
2.1 GCNT3在癌旁正常组织和肺腺癌组织中的表达情况
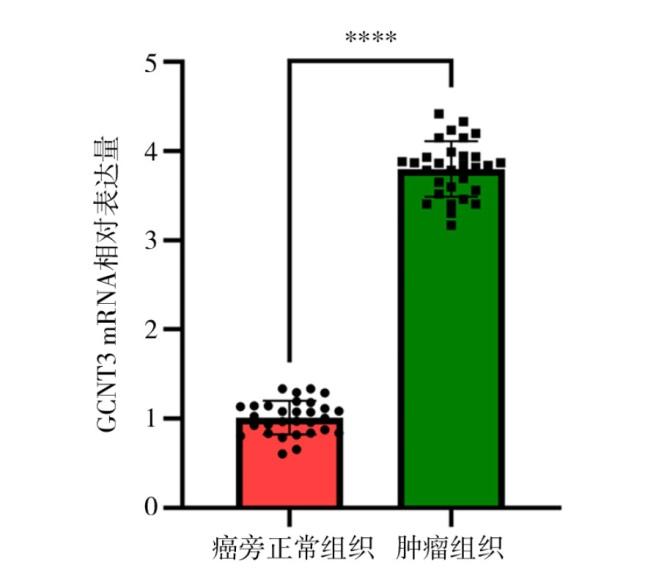
RT-qPCR法结果显示,癌旁正常组织中GCNT3 mRNA的表达量为1.00±0.23,而肺腺癌组织中GCNT3 mRNA的表达量为3.75±0.28,差异具有统计学意义(t = 41.57,P < 0.000 1)。见图1。
2.2 下调GCNT3对肺腺癌H1650细胞增殖水平的影响
CCK-8法检测结果显示,Sh NC组在24、48和72 h的增殖率分别为(57.64±3.96)%、(76.26±4.58)%和(92.24±5.12)%;Sh GCNT3组在相应时间点的增殖率分别为(42.32±3.72)%、(62.21±4.62)%和(73.31±4.86)%。组间的增殖率比较差异均有统计学意义(均P < 0.05)。见表1。
表1 下调GCNT3对肺腺癌H1650细胞增殖水平的影响Table 1 The effect of downregulating GCNT3 on the proliferation level of lung adenocarcinoma H1650 cells |
| 组 别 | n | 细胞增殖率/% | ||
|---|---|---|---|---|
| 24 h | 48 h | 72 h | ||
| Sh NC组 | 3 | 57.64±3.96 | 76.26±4.58 | 92.24±5.12 |
| Sh GCNT3组 | 3 | 42.32±3.72 | 62.21±4.62 | 73.31±4.86 |
| t值 | -4.88 | -3.74 | -4.64 | |
| P值 | 0.008 | 0.020 | 0.010 | |
2.3 下调GCNT3对肺腺癌H1650细胞凋亡水平的影响
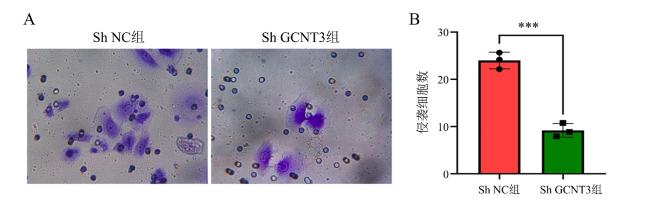
2.4 下调GCNT3对肺腺癌PC3细胞侵袭水平的影响
Transwell实验结果显示,2组侵袭细胞数分别为(25.12±2.30)个与(9.26±1.68)个,Sh GCNT3组细胞的侵袭能力低于Sh NC组,差异有统计学意义(t = -9.64,P < 0.001)。见图3。
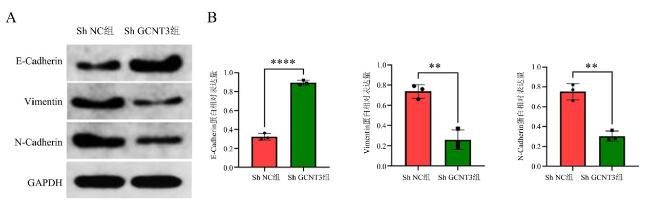
2.5 下调GCNT3对肺腺癌PC3细胞上皮-间质转化表型的影响
蛋白免疫印迹法结果显示,与NC组(0.33±0.06)比较,Sh GCNT3组E-cadherin蛋白(0.85±0.07)表达水平增加,差异有统计学意义(t = 9.77,P < 0.001);与NC组(0.72±0.06,0.72±0.05)比较,Sh GCNT3组Vimentin、N-cadherin蛋白(0.31±0.05,0.32±0.04)表达水平降低,差异均有统计学意义(t = -9.09,P < 0.001;t = -9.61,P < 0.001)。见图4。
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
3 讨论
根据近年的全球癌症统计数据,肺癌仍然是导致癌症相关死亡的首要原因,约占全球癌症死亡人数的18%[19-21]。在中国,肺癌也是癌症病死率最高的肿瘤类型,病死率达19%,这一趋势可能与吸烟年轻人群中肺癌发病率的增加密切相关[22-25]。尽管近年来手术、放射治疗、化学治疗及靶向治疗等治疗手段取得了显著进展,肺癌患者的整体预后依然不甚理想,特别是在具有转移、复发及治疗耐药性的患者中[26-30]。肺腺癌是肺癌的一种,属于非小细胞癌。不同于鳞状细胞肺癌,肺腺癌较多见于女性及抽烟者。其起源于支气管黏膜上皮,少数起源于大支气管的黏液腺,其预后优于其他类型的肺癌[31]。探讨肺腺癌放射治疗耐药的机制和潜在分子靶点,对更好地改善患者的生存预后具有重要意义[32]。
本研究首先通过RT-qPCR检测了30例肺腺癌及其癌旁正常组织中GCNT3的表达水平,结果显示肺腺癌组织中GCNT3表达高于癌旁正常组织,提示GCNT3可能与肺腺癌的发生密切相关。为进一步探究GCNT3在肺腺癌进展中的作用机制,本研究通过转染GCNT3 ShRNA构建了GCNT3敲低的H1650细胞株,评估了GCNT3的下调对肺腺癌相关恶性生物学行为的影响。结果表明,GCNT3的敲低抑制了H1650细胞的增殖,同时促进了细胞凋亡,这一过程进一步导致了细胞侵袭能力的降低。研究结果表明,GCNT3在调控细胞生长和生存中发挥着关键作用,可能通过影响细胞的生存和迁移机制,协调细胞增殖与凋亡的平衡。因此,GCNT3的表达可能是维持H1650细胞增殖与侵袭能力的重要因素。
EMT是一种细胞通过特定程序由上皮表型转化为间质表型的生物学过程,在肿瘤发展、创伤修复、胚胎发育及器官纤维化过程中具有重要作用[40-42]。EMT通常伴随着上皮细胞黏附分子E-cadherin表达的下调及间质标志物Vimentin的上调,目前被公认是推动肺腺癌转移的重要机制[43-45]。大部分肿瘤细胞中的E-Cadherin的表达是下调的,而N-Cadherin的表达增加[46]。本研究进一步通过蛋白免疫印迹法发现,敲低GCNT3表达水平能够抑制H1650细胞E-cadherin表达的下调、间质标志物Vimentin的上调,而N-Cadherin的表达增加,这表明GCNT3可能通过调控EMT过程促进肺腺癌的侵袭和转移。
综上所述,本研究证实了GCNT3在肺腺癌中的高表达,并通过调控H1650细胞的增殖、侵袭、凋亡及EMT过程,表明GCNT3在肺腺癌的发生、发展中起到至关重要的作用。GCNT3有望作为肺腺癌诊断和治疗的潜在靶点,尤其是在阻止肺腺癌转移方面具有重要的应用前景。
利益冲突声明:本研究未受到企业、公司等第三方资助,不存在潜在利益冲突。