 PDF(2108 KB)
PDF(2108 KB)
 PDF(2108 KB)
PDF(2108 KB)
 PDF(2108 KB)
PDF(2108 KB)
3D打印技术辅助腹主动脉瘤腔内治疗一例
3D printing-assisted intraluminal treatment of abdominal aortic aneurysm: a case report
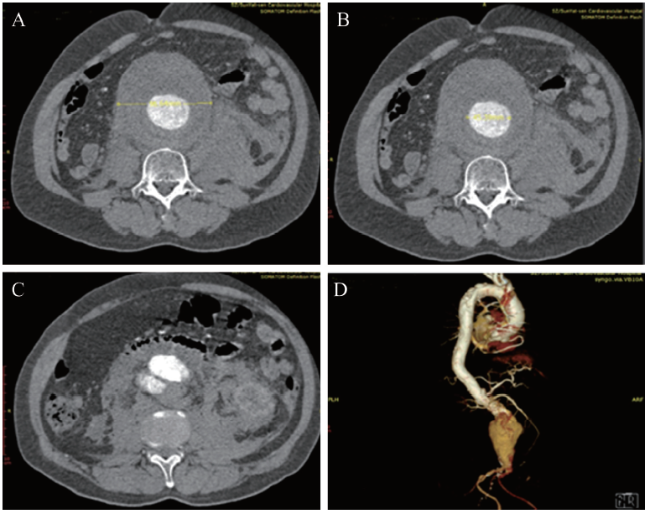
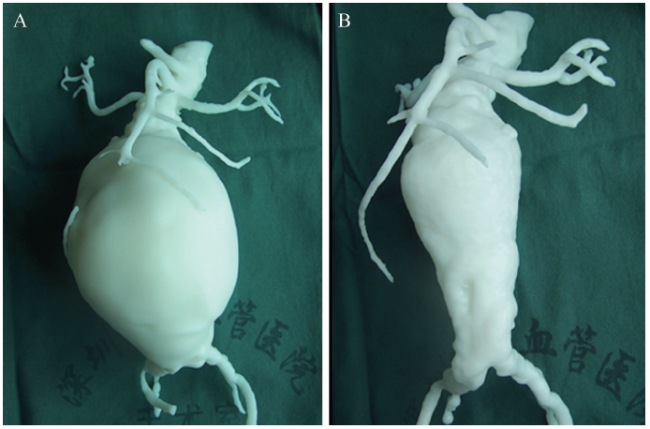
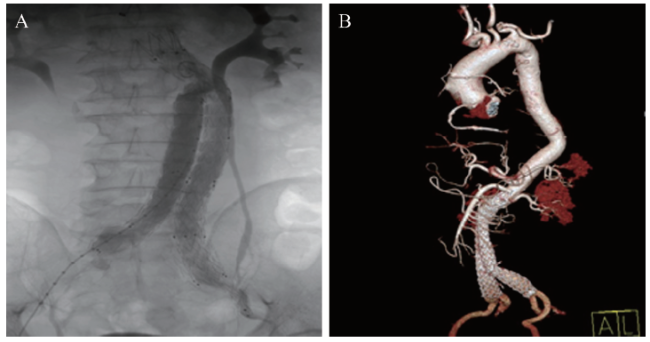
腹主动脉瘤是指与全身纤维结缔组织退行性变相关联的腹主动脉局部瘤样扩张,是常见的主动脉疾病。近年随着三维(3D)打印技术的不断进步,其在医疗领域应用的范围不断扩大,特别是在血管外科的运用。该文介绍1例腹主动脉瘤3D打印辅助治疗实例,与传统主动脉CT血管造影(CTA)检查进行对比,基于CTA图像的3D打印技术能够精准地还原CTA重建图像,测量数据更客观,使外科医师获得更直观的视觉理解,有助于手术的顺利进行。
Abdominal aortic aneurysm refers to the local tumor-like dilatation of the abdominal aorta associated with the degeneration of systemic fibrous connective tissues, which is a common type of aortic disease. In recent years, with the persistent advancement of three-dimensional (3D) printing technology, its range of application in the medical field has been constantly expanded, especially in vascular surgery. In this article, one case of 3D printing-assisted treatment of abdominal aortic aneurysm was reported. Compared with traditional aortic CT angiography (CTA), 3D printing technology based on CTA image can more accurately restore the reconstructed CTA image, yield more objective measurement data, deliver more intuitive visual understanding to the surgeons and contribute to the success of surgery.
腹主动脉瘤 / 腔内治疗 / 三维打印 {{custom_keyword}} /
Abdominal aortic aneurysm / Intraluminal treatment / Three-dimensional printing {{custom_keyword}} /
表1 腹主动脉瘤CTA测量与3D模型测量之间对比 |
| 项 目 | CT图像测量 | 3D模型测量 |
|---|---|---|
| 左肾动脉下缘瘤颈长度(mm) | 18.3 | 18.7 |
| 右肾动脉下缘瘤颈长度(mm) | 44.0 | 44.5 |
| 瘤颈最大直径(mm) | 22.5 | 22.0 |
| 瘤腔最大直径(mm) | 56.4 | 55.0 |
| a角(°) | 14 | 14 |
| b角(°) | 45 | 47 |
| 瘤体最大直径(mm) | 99.9 | 99.0 |
| 左肾动脉开口直径(mm) | 5.9 | 6.2 |
| 右肾动脉开口直径(mm) | 3.5 | 3.7 |
| 左侧髂总动脉开口直径(mm) | 12.2 | 11.0 |
| 右侧髂总动脉开口直径(mm) | 16.7 | 15.8 |
| 腹主动脉瘤体长度(mm) | 105.0 | 107.0 |
| 注:a角为瘤颈与正常腹主动脉夹角;b角为瘤颈与腹主动脉中轴夹角 |
| [1] |
黄建华, 王伟. 3D打印技术在腔内血管外科中的应用前景. 临床外科杂志, 2015,23(8):577-579.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [2] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [3] |
林若然, 吕俊远, 辛世杰. 3D打印技术在血管外科应用进展. 中国实用外科杂志, 2016,36(12):1338-1340.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [4] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [5] |
刘继峰, 郭旺明. 多层螺旋CT血管成像在腹主动脉瘤诊断及术前评估中的应用价值. 中国医疗设备, 2015,30(9):60-62.
目的 探讨多层螺旋CT血管成像(CTA)在腹主动脉瘤诊断及术前评估中的应用价值。方法选择经手术或数字减影血管造影(DSA)证实的82例腹主动脉瘤患者作为研究对象。采用CTA技术对患者的腹主动脉及其分支进行扫描,应用多平面重建、最大密度投影、容积成像等技术对图像进行重建,并进行分型、病灶位置和累及范围等定位。结果 82例腹主动脉瘤中,CTA检出76例,与DSA检查结果相比,差异无统计学意义(P>0.05)。CTA评估Ⅰ型8例、ⅡA型7例、ⅡB型9例、ⅡC型40例、Ⅲ型12例,近肾型10例,肾下型66例,与DSA检查结果相比,差异无统计学意义(P>0.05)。结论 CTA技术对腹主动脉瘤具有较高的诊断准确率,可准确评估瘤体的形态、部位、大小,指导临床治疗方案的选择及手术指征的确定。
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [6] |
杨晗, 胡明, 黄群, 覃忠, 郭思恩, 覃晓. 3D打印辅助覆膜支架修复术在复杂主动脉疾病腔内治疗中的应用. 中国血管外科杂志(电子版), 2018,10(1):4-9.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [7] |
The purpose of this article is to review recent innovations on the process and application of 3-dimensional (3D) printed objects from medical imaging data. Data for 3D printed medical models can be obtained from computed tomography, magnetic resonance imaging, and ultrasound using the Data Imaging and Communications in Medicine (DICOM) software. The data images are processed using segmentation and mesh generation tools and converted to a standard tessellation language (STL) file for printing. 3D printing technologies include stereolithography, selective laser sintering, inkjet, and fused-deposition modeling . 3D printed models have been used for preoperative planning of complex surgeries, the creation of custom prosthesis, and in the education and training of physicians. The application of medical imaging and 3D printers has been successful in providing solutions to many complex medical problems. As technology advances, its applications continue to grow in the future.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [8] |
Rapid prototyping, also known as three-dimensional (3D) printing, is a recent technologic advancement with tremendous potential for advancing medical device design. A wide range of raw materials can be incorporated into complex 3D structures, including plastics, metals, biocompatible polymers, and even living cells. With its promise of highly customized, adaptable, and personalized device design at the point of care, 3D printing stands to revolutionize medical care. The present review summarizes the methods for 3D printing and their current and potential roles in medical device design, with an emphasis on their potential relevance to interventional radiology.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [9] |
3D-printed models fabricated from CT, MRI, or echocardiography data provide the advantage of haptic feedback, direct manipulation, and enhanced understanding of cardiovascular anatomy and underlying pathologies. Reported applications of cardiovascular 3D printing span from diagnostic assistance and optimization of management algorithms in complex cardiovascular diseases, to planning and simulating surgical and interventional procedures. The technology has been used in practically the entire range of structural, valvular, and congenital heart diseases, and the added-value of 3D printing is established. Patient-specific implants and custom-made devices can be designed, produced, and tested, thus opening new horizons in personalized patient care and cardiovascular research. Physicians and trainees can better elucidate anatomical abnormalities with the use of 3D-printed models, and communication with patients is markedly improved. Cardiovascular 3D bioprinting and molecular 3D printing, although currently not translated into clinical practice, hold revolutionary potential. 3D printing is expected to have a broad influence in cardiovascular care, and will prove pivotal for the future generation of cardiovascular imagers and care providers. In this Review, we summarize the cardiovascular 3D printing workflow, from image acquisition to the generation of a hand-held model, and discuss the cardiovascular applications and the current status and future perspectives of cardiovascular 3D printing.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [10] |
While use of advanced visualization in radiology is instrumental in diagnosis and communication with referring clinicians, there is an unmet need to render Digital Imaging and Communications in Medicine (DICOM) images as three-dimensional (3D) printed models capable of providing both tactile feedback and tangible depth information about anatomic and pathologic states. Three-dimensional printed models, already entrenched in the nonmedical sciences, are rapidly being embraced in medicine as well as in the lay community. Incorporating 3D printing from images generated and interpreted by radiologists presents particular challenges, including training, materials and equipment, and guidelines. The overall costs of a 3D printing laboratory must be balanced by the clinical benefits. It is expected that the number of 3D-printed models generated from DICOM images for planning interventions and fabricating implants will grow exponentially. Radiologists should at a minimum be familiar with 3D printing as it relates to their field, including types of 3D printing technologies and materials used to create 3D-printed anatomic models, published applications of models to date, and clinical benefits in radiology. Online supplemental material is available for this article.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [11] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [12] |
OBJECTIVE: The objective of this study is to verify the accuracy of 3D-printed hollow models of visceral aneurysms created from CT angiography (CTA) data, by evaluating the sizes and shapes of aneurysms and related arteries. SUBJECTS AND METHODS: From March 2006 to August 2015, 19 true visceral aneurysms were embolized via interventional radiologic treatment provided by the radiology department at our institution; aneurysms with bleeding (n = 3) or without thin-slice (< 1="" mm="" preembolization="" ct="" data="" n="1)" were="" excluded.="" a="" total="" of="" 15="" consecutive="" true="" visceral="" aneurysms="" from="" 11="" patients="" eight="" women="" and="" three="" men="" mean="" age="" 61="" years="" range="" 53-72="" years="" whose="" aneurysms="" were="" embolized="" via="" endovascular="" procedures="" were="" included="" in="" this="" study.="" three-dimensional-printed="" hollow="" models="" of="" aneurysms="" and="" related="" arteries="" were="" fabricated="" from="" cta="" data.="" the="" accuracies="" of="" the="" sizes="" and="" shapes="" of="" the="" 3d-printed="" hollow="" models="" were="" evaluated="" using="" the="" nonparametric="" wilcoxon="" signed="" rank="" test="" and="" the="" dice="" coefficient="" index.="" results:="" aneurysm="" sizes="" ranged="" from="" 138="" to="" 18691="" mm3="" diameter="" 6.1-35.7="" mm="" and="" no="" statistically="" significant="" difference="" was="" noted="" between="" patient="" data="" and="" 3d-printed="" models="" p="0.56)." shape="" analysis="" of="" whole="" aneurysms="" and="" related="" arteries="" indicated="" a="" high="" level="" of="" accuracy="" dice="" coefficient="" index="" value="" 84.2-95.8="" mean="" -="" sd="" 91.1="" -="" 4.1.="" conclusion:="" the="" sizes="" and="" shapes="" of="" 3d-printed="" hollow="" visceral="" aneurysm="" models="" created="" from="" cta="" data="" were="" accurate.="" these="" models="" can="" be="" used="" for="" simulations="" of="" endovascular="" treatment="" and="" precise="" anatomic="" information.="">
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [13] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [14] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [15] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [16] |
OBJECTIVE: The fenestrated Anaconda endograft (Vascutek/Terumo, Inchinnan, UK) is intended for the treatment of abdominal aortic aneurysms with an insufficient infrarenal landing zone. The endografts are custom-made with use of high-resolution, 1-mm-slice computed tomography angiography images. For every case, a nonsterile prototype and a three-dimensional (3D) model of the patient's aorta are constructed to allow the engineers as well as the physician to test-implant the device and to review the fit of the graft. The aim of this investigation was to assess the impact of 3D model construction and prototype testing on the design of the final sterile endograft. METHODS: A prospectively held database on fenestrated endovascular aortic repair patients treated at a single institution was completed with data from the Vascutek engineers' prototype test results as well as the product request forms. Changes to endograft design based on prototype testing were assessed and are reported for all procedures. RESULTS: Between April 1, 2013, and August 18, 2015, 60 fenestrated Anaconda devices were implanted. Through prototype testing, engineers were able to identify and report potential risks to technical success related to use of the custom device for the respective patient. Theoretical concerns about endograft fit in the rigid model were expressed in 51 cases (85.0%), and the engineers suggested potential changes to the design of 21 grafts (35.0%). Thirteen cases (21.7%) were eventually modified after the surgeon's testing of the prototype. A second prototype was ordered in three cases (5.0%) because of extensive changes to endograft design, such as inclusion of an additional fenestration. Technical success rates were comparable for grafts that showed a perfect fit from the beginning and cases in which prototype testing resulted in a modification of graft design. CONCLUSIONS: Planning and construction of fenestrated endografts for complex aortic anatomies where exact fit and positioning of the graft are paramount to allow cannulation of the aortic branches are challenging. In the current series, approximately one in five endografts was modified after prototype testing in an aortic model. Eventually, success rates were comparable between the groups of patients with a good primary prototype fit and those in which the endograft design was altered. Prototype testing in 3D aortic models is a valuable tool to test the fit of a custom-made endograft before implantation. This may help avoid potentially debilitating adverse events associated with misaligned fenestrations and unconnected aortic branches.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [17] |
United Kingdom EVAR Trial Investigators,
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [18] |
BACKGROUND: Endovascular aneurysm repair (EVAR) is a new technology to treat patients with abdominal aortic aneurysm (AAA) when the anatomy is suitable. Uncertainty exists about how endovascular repair compares with conventional open surgery. EVAR trial 1 was instigated to compare these treatments in patients judged fit for open AAA repair. METHODS: Between 1999 and 2003, 1082 elective (non-emergency) patients were randomised to receive either EVAR (n=543) or open AAA repair (n=539). Patients aged at least 60 years with aneurysms of diameter 5.5 cm or more, who were fit enough for open surgical repair (anaesthetically and medically well enough for the procedure), were recruited for the study at 41 British hospitals proficient in the EVAR technique. The primary outcome measure is all-cause mortality and these results will be released in 2005. The primary analysis presented here is operative mortality by intention to treat and a secondary analysis was done in per-protocol patients. FINDINGS: Patients (983 men, 99 women) had a mean age of 74 years (SD 6) and mean AAA diameter of 6.5 cm (SD 1). 1047 (97%) patients underwent AAA repair and 1008 (93%) received their allocated treatment. 30-day mortality in the EVAR group was 1.7% (9/531) versus 4.7% (24/516) in the open repair group (odds ratio 0.35 [95% CI 0.16-0.77], p=0.009). By per-protocol analysis, 30-day mortality for EVAR was 1.6% (8/512) versus 4.6% (23/496) for open repair (0.33 [0.15-0.74], p=0.007). Secondary interventions were more common in patients allocated EVAR (9.8% vs 5.8%, p=0.02). INTERPRETATION: In patients with large AAAs, treatment by EVAR reduced the 30-day operative mortality by two-thirds compared with open repair. Any change in clinical practice should await durability and longer term results.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [19] |
PURPOSE: To describe rapid prototyping or 3-dimensional (3D) printing of aneurysms with complex neck anatomy to facilitate endovascular aneurysm repair (EVAR). CASE REPORT: A 75-year-old man had a 6.6-cm infrarenal aortic aneurysm that appeared on computed tomographic angiography to have a sharp neck angulation of ~90 degrees . However, although the computed tomography (CT) data were analyzed using centerline of flow, the true neck length and relations of the ostial origins were difficult to determine. No multidisciplinary consensus could be reached as to which stent-graft to use owing to these borderline features of the neck anatomy. Based on past experience with rapid prototyping technology, a decision was taken to print a model of the aneurysm to aid in visualization of the neck anatomy. The CT data were segmented, processed, and converted into a stereolithographic format representing the lumen as a 3D volume, from which a full-sized replica was printed within 24 hours. The model demonstrated that the neck was adequate for stent-graft repair using the Aorfix device. CONCLUSION: Rapid prototyping of aortic aneurysms is feasible and can aid decision making and device delivery. Further work is required to test the value of 3D replicas in planning procedures and their impact on procedure time, radiation dose, and procedure cost.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [20] |
OBJECTIVE: The fenestrated Anaconda endograft (Vascutek/Terumo, Inchinnan, UK) is intended for the treatment of abdominal aortic aneurysms with an insufficient infrarenal landing zone. The endografts are custom-made with use of high-resolution, 1-mm-slice computed tomography angiography images. For every case, a nonsterile prototype and a three-dimensional (3D) model of the patient's aorta are constructed to allow the engineers as well as the physician to test-implant the device and to review the fit of the graft. The aim of this investigation was to assess the impact of 3D model construction and prototype testing on the design of the final sterile endograft. METHODS: A prospectively held database on fenestrated endovascular aortic repair patients treated at a single institution was completed with data from the Vascutek engineers' prototype test results as well as the product request forms. Changes to endograft design based on prototype testing were assessed and are reported for all procedures. RESULTS: Between April 1, 2013, and August 18, 2015, 60 fenestrated Anaconda devices were implanted. Through prototype testing, engineers were able to identify and report potential risks to technical success related to use of the custom device for the respective patient. Theoretical concerns about endograft fit in the rigid model were expressed in 51 cases (85.0%), and the engineers suggested potential changes to the design of 21 grafts (35.0%). Thirteen cases (21.7%) were eventually modified after the surgeon's testing of the prototype. A second prototype was ordered in three cases (5.0%) because of extensive changes to endograft design, such as inclusion of an additional fenestration. Technical success rates were comparable for grafts that showed a perfect fit from the beginning and cases in which prototype testing resulted in a modification of graft design. CONCLUSIONS: Planning and construction of fenestrated endografts for complex aortic anatomies where exact fit and positioning of the graft are paramount to allow cannulation of the aortic branches are challenging. In the current series, approximately one in five endografts was modified after prototype testing in an aortic model. Eventually, success rates were comparable between the groups of patients with a good primary prototype fit and those in which the endograft design was altered. Prototype testing in 3D aortic models is a valuable tool to test the fit of a custom-made endograft before implantation. This may help avoid potentially debilitating adverse events associated with misaligned fenestrations and unconnected aortic branches.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [21] |
BACKGROUND: Three-dimensional (3D) printing is a manufacturing process in which an object is created by specialist printers designed to print in additive layers to create a 3D object. Whilst there are initial promising medical applications of 3D printing, a lack of evidence to support its use remains a barrier for larger scale adoption into clinical practice. Endovascular virtual reality (VR) simulation plays an important role in the safe training of future endovascular practitioners, but existing VR models have disadvantages including cost and accessibility which could be addressed with 3D printing. METHODS: This study sought to evaluate the feasibility of 3D printing an anatomically accurate human aorta for the purposes of endovascular training. RESULTS: A 3D printed model was successfully designed and printed and used for endovascular simulation. The stages of development and practical applications are described. Feedback from 96 physicians who answered a series of questions using a 5 point Likert scale is presented. CONCLUSIONS: Initial data supports the value of 3D printed endovascular models although further educational validation is required.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [22] |
BACKGROUND: Imaging has a critical impact on surgical decision making and three-dimensional (3D) digital models of patient pathology can now be made commercially. We developed a 3D digital model of a cancer of the head of the pancreas by integrating actual CT data with 3D modeling process. After this process, the virtual pancreatic model was also produced using a high-quality 3D printer. PATIENTS AND METHODS: A 56-year-old female with pancreatic head adenocarcinoma presented with biliary obstruction and jaundice. The CT scan showed a borderline resectable tumor with a clear involvement of the gastroduodenal artery but doubtful relationships with the hepatic artery. Our team in collaboration with the Immersive Touch team used multiple series from the CT and segmented the relevant anatomy to understand the physical location of the tumor. An STL file was then developed and printed. RESULTS: Reconstructing and compositing the different series together enhanced the imaging, which allowed clearer observations of the relationship between the mass and the blood vessels, and evidence that the tumor was unresectable. Data files were converted for printing a 100% size rendering model, used for didactic purposes and to discuss with the patient. CONCLUSIONS: This study showed that (1) reconstructing enhanced traditional imaging by merging and modeling different series together for a 3D view with diverse angles and transparency, allowing the observation of previously unapparent anatomical details; (2) with this new technology surgeons and residents can preobserve their planned surgical intervention, explore the patient-specific anatomy, and sharpen their procedure choices; (3) high-quality 3D printed models are increasingly useful not only in the clinical realm but also for personalized patient education.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [23] |
BACKGROUND: With the increasing application of fenestrated and physician-modified endografting for aneurysm repair, there is increasing concern about the accuracy of vessel position measurements based on computed tomography scans. Inaccuracies in measurements may result in a
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [24] |
OBJECTIVE: To assess the effect of patient-specific virtual reality rehearsal (PsR) before endovascular infrarenal aneurysm repair (EVAR) on technical performance and procedural errors. BACKGROUND: Endovascular procedures, including EVAR, are executed in a complex multidisciplinary environment, often treating high-risk patients. Consequently, this may lead to patient harm and procedural inefficiency. PsR enables the endovascular team to evaluate and practice the case in a virtual environment before treating the real patient. METHODS: A multicenter, prospective, randomized controlled trial recruited 100 patients with a nonruptured infrarenal aortic or iliac aneurysm between September 2012 and June 2014. Cases were randomized to preoperative PsR or standard care (no PsR). Primary outcome measures were errors during the real procedure and technical operative metrics (total endovascular and fluoroscopy time, contrast volume, number of angiograms, and radiation dose). RESULTS: There was a 26% [95% confidence interval (CI) 9%-40%, P = 0.004) reduction in minor errors, a 76% (95% CI 30%-92%, P = 0.009) reduction in major errors, and a 27% (95% CI 8.2%-42%, P = 0.007) reduction in errors causing procedural delay in the PsR group. The number of angiograms performed to visualize proximal and distal landing zones was 23% (95% CI 8%-36%, P = 0.005) and 21% (95% CI 7%-32%, P = 0.004) lower in the PsR group. CONCLUSIONS: PsR before EVAR can be used in different hospital settings by teams with various EVAR experience. It reduces perioperative errors and the number of angiograms required to deploy the stent graft, thereby reducing delays. Ultimately, it may improve patient safety and procedural efficiency.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [25] |
OBJECTIVE: Detailed 3-dimensional anatomic information is essential when planning strategies of surgical treatment for patients with complex congenitally malformed hearts. Current imaging techniques, however, do not always provide all the necessary anatomic information in a user-friendly fashion. We sought to assess the practical clinical value of realistic 3-dimensional models of complex congenitally malformed hearts. METHODS: In 11 patients, aged from 0.8 to 27 years, all with complex congenitally malformed hearts, an unequivocal decision regarding the optimum surgical strategy had not been reached when using standard diagnostic tools. Therefore, we constructed 3-dimensional virtual computer and printed cast models of the heart on the basis of high-resolution whole-heart or cine magnetic resonance imaging or computed tomography. Anatomic descriptions were compared with intraoperative findings when surgery was performed. RESULTS: Independently of age-related factors, images acquired in all patients using magnetic resonance imaging and computed tomography proved to be of sufficient quality for producing the models without major differences in the postprocessing and revealing the anatomy in an unequivocal 3-dimensional context. Examination of the models provided invaluable additional information that supported the surgical decision-making. The anatomy as shown in the models was confirmed during surgery. Biventricular corrective surgery was achieved in 5 patients, palliative surgery was achieved in 3 patients, and lack of suitable surgical options was confirmed in the remaining 3 patients. CONCLUSION: Realistic 3-dimensional modeling of the heart provides a new means for the assessment of complex intracardiac anatomy. We expect this method to change current diagnostic approaches and facilitate preoperative planning.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [26] |
BACKGROUND: Structural heart disease, including valvular disease as well as congenital defects, causes important alterations in heart anatomy. As a result, individualised planning for both surgical and percutaneous procedures is crucial for procedural optimisation. Three dimensional (3D) rapid prototyping techniques are being utilised to aid operators in planning structural heart procedures. AIM: We intend to provide a description of 3D printing as a clinically applicable heart modelling technology for the planning of percutaneous structural heart procedures as well as to report our first clinical use of a 3D printed patient-specific heart model in preparation for a percutaneous mitral annuloplasty using the Mitralign percutaneous annuloplasty system. METHODS: Retrospectively gated, contrast enhanced, multi-slice computed tomography (MSCT) scans were obtained. MSCT DICOM data was analysed using software that creates 3D surface files of the blood volume of specific regions of interest in the heart. The surface files are rendered using a software package that creates a solid model that can be printed using commercially available stereolithography machines. RESULTS: The technique of direct percutaneous mitral annuloplasty requires advancement of a guiding catheter through the aorta, into the left ventricle, and requires the positioning of the tip of the catheter between the papillary muscles in close proximity to the mitral annulus. The 3D heart model was used to create a procedural plan to optimise potential device implantation. The size of the deflectable guiding catheter was selected on the basis of the patient's heart model. Target locations for annulus crossing wires were evaluated pre-procedurally using the individual patient's 3D heart model. In addition, the ability to position the Bident Catheter at the appropriate locations under the mitral annulus as well as the manoeuvrability between the papillary muscles were analysed on the heart model, enabling safe completion of the procedure, which resulted in a significant reduction in mitral regurgitation. CONCLUSIONS: 3D printing is a helpful tool in individualised planning for percutaneous structural interventions. Future studies are warranted to assess its role in preparing for percutaneous and surgical heart procedures.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| {{custom_ref.label}} |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
PDF(2108 KB)
/
| 〈 |
|
〉 |





{kind=link}
{kind=link}
{kind=link}