 PDF(1507 KB)
PDF(1507 KB)

过敏性疾病共病和多病多学科诊疗模式——以中山大学附属第三医院过敏科为例
周琪琳, 谭静芊, 粟静, 成昀, 熊国威, 周敏, 郑瑞, 张昆, 戴敏, 张萍萍, 黎雅婷, 黄雪琨, 石照辉, 张雅娜, 甘照宇, 陶金, 许成芳, 周宇麒, 冯佩英, 陈壮桂, 杨钦泰
新医学 ›› 2024, Vol. 55 ›› Issue (10) : 757-763.
PDF(1507 KB)
 PDF(1507 KB)
PDF(1507 KB)
过敏性疾病共病和多病多学科诊疗模式——以中山大学附属第三医院过敏科为例
Multi-disciplinary diagnosis and treatment mode for allergic comorbidity and multimorbidity: take the Department of Allergy of the Third Affiliated Hospital of Sun Yat-sen University as an example
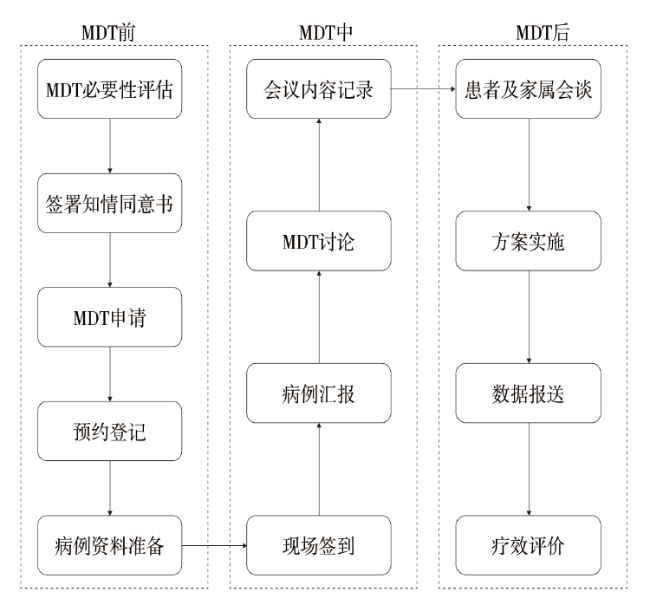
过敏性疾病的发病率呈上升趋势,多系统过敏性疾病往往共同并发于同一患者身上,如何高质高效、合理规范地进行综合诊疗十分重要。多学科诊疗为复杂难治的过敏性疾病共病和多病提供了新的解决途径,是对传统分科诊疗模式的有效补充,也是过敏性疾病诊疗发展的趋势。目前国内外有关过敏性疾病共病和多病多学科诊疗还处于探索阶段,尚未形成成熟的体系和运行模式。文章结合中山大学附属第三医院过敏性疾病专家团队的临床探索和实践经验,从实施目标、组织结构、基本要求、运行模式、步骤流程、制度保障、质量控制等方面阐述过敏性疾病共病和多病多学科诊疗体系的构建与实施,从而提高过敏性疾病共病和多病多学科诊疗的水平。
The incidence of allergic diseases is gradually increasing, and multi-system allergic diseases often co-occur in the same patient. It is very important to conduct comprehensive diagnosis and treatment with high quality, high efficiency, reasonable and standardized. The multi-disciplinary diagnosis and treatment provides a new way to solve the complicated and difficult comorbidities of allergic comorbidity and multimorbidity, which is an effective supplement to the traditional diagnosis and treatment mode, and is also the development trend of the diagnosis and treatment of allergic diseases. At present, the multi-disciplinary treatment of allergic comorbidity and multimorbidity is still in the exploratory stage at home and abroad, and has not yet formed a mature system or a operation mode. Based on the clinical exploration and practical experience of allergic disease expert team of the Third Affiliated Hospital of Sun Yat-sen University, this paper expounds the construction and implementation of the multi-disciplinary treatment system for allergic comorbidity and multimorbidity from the aspects of implementation objectives, organizational structure, basic requirements, operation mode, procedure, system guarantee, quality control and so on. Establishing a standardized, mature and perfect multi-disciplinary treatment system for allergic comorbidity and multimorbidity and ensuring its effective operation and implementation will help to improve the level of multi-disciplinary diagnosis and treatment for allergic comorbidity and multimorbidity.
过敏 / 过敏性疾病共病和多病 / 多学科诊疗 / 过敏管理 {{custom_keyword}} /
Allergy / Allergic comorbidity and multimorbidity / Multi-disciplinary diagnosis and treatment / Allergy management {{custom_keyword}} /

| [1] |
张萍萍, 杨丽芬, 梁英, 等. 儿童变应原免疫治疗的临床应用进展[J]. 新医学, 2022, 53(2): 87-92. DOI: 10.3969/j.issn.0253-9802.2022.02.003.
变应原免疫治疗(AIT)是通过诱导过敏原特异性免疫耐受来改变过敏性疾病进程的唯一对因治疗方法。尽管已有大量的临床试验和荟萃分析证实AIT的安全性及有效性,但其仍未得到广泛应用。全球正在不断开发AIT变应原制剂及探索AIT治疗策略,大部分现有临床数据来自成人,儿童数据匮乏,亟需推进儿童过敏性疾病的诊疗规范化、制定统一的AIT策略。该文就目前儿童AIT领域的进展情况作一综述,以期为更深入的研究提供参考。
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [2] |
Environmental exposures interplay with human host factors to promote the development and progression of allergic diseases. The worldwide prevalence of allergic disease is rising as a result of complex gene-environment interactions that shape the immune system and host response. Research shows an association between the rise of allergic diseases and increasingly modern Westernized lifestyles, which are characterized by increased urbanization, time spent indoors, and antibiotic usage. These environmental changes result in increased exposure to air and traffic pollution, fungi, infectious agents, tobacco smoke, and other early-life and lifelong risk factors for the development and exacerbation of asthma and allergic diseases. It is increasingly recognized that the timing, load, and route of allergen exposure affect allergic disease phenotypes and development. Still, our ability to prevent allergic diseases is hindered by gaps in understanding of the underlying mechanisms and interaction of environmental, viral, and allergen exposures with immune pathways that impact disease development. This Review highlights epidemiologic and mechanistic evidence linking environmental exposures to the development and exacerbation of allergic airway responses.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [3] |
叶丽妍, 曾丽盈, 陈佩文, 等. 参苓白术散早期干预对与噁唑酮诱导过敏性结肠炎幼鼠的影响[J]. 暨南大学学报(自然科学与医学版), 2022, 43(4): 361-372. DOI: 10.11778/j.jdxb.20210300.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [4] |
张娜娜, 曹华, 万毅新. 支气管热成形术治疗难治性哮喘研究进展[J]. 中国医学物理学杂志, 2019, 36(1): 108-111. DOI: 10.3969/j.issn.1005-202X.2019.01.021.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [5] |
The atopic march recognizes the increased occurrence of asthma, allergic rhinitis, or both after atopic dermatitis (AD) onset. Mechanisms for developing atopic comorbidities after AD onset are poorly understood but can involve the impaired cutaneous barrier, which facilitates cutaneous sensitization. The association can also be driven or amplified in susceptible subjects by a systemic T2-dominant immune response to cutaneous inflammation. However, these associations might merely involve shared genetic loci and environmental triggers, including microbiome dysregulation, with the temporal sequence reflecting tissue-specific peak time of occurrence of each disease, suggesting more of a clustering of disorders than a march. Prospective longitudinal cohort studies provide an opportunity to explore the relationships between postdermatitis development of atopic disorders and potential predictive phenotypic, genotypic, and environmental factors. Recent investigations implicate disease severity and persistence, age of onset, parental atopic history, filaggrin (FLG) mutations, polysensitization, and the nonrural environment among risk factors for development of multiple atopic comorbidities in young children with AD. Early intervention studies to repair the epidermal barrier or alter exposure to the microbiome or allergens might elucidate the relative roles of barrier defects, genetic locus alterations, and environmental exposures in the risk and sequence of occurrence of T2 activation disorders.Copyright © 2018 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [6] |
Atopic dermatitis is a common inflammatory skin disorder characterised by recurrent eczematous lesions and intense itch. The disorder affects people of all ages and ethnicities, has a substantial psychosocial impact on patients and relatives, and is the leading cause of the global burden from skin disease. Atopic dermatitis is associated with increased risk of multiple comorbidities, including food allergy, asthma, allergic rhinitis, and mental health disorders. The pathophysiology is complex and involves a strong genetic predisposition, epidermal dysfunction, and T-cell driven inflammation. Although type-2 mechanisms are dominant, there is increasing evidence that the disorder involves multiple immune pathways. Currently, there is no cure, but increasing numbers of innovative and targeted therapies hold promise for achieving disease control, including in patients with recalcitrant disease. We summarise and discuss advances in our understanding of the disease and their implications for prevention, management, and future research.Copyright © 2020 Elsevier Ltd. All rights reserved.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [7] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [8] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [9] |
Host-microbiota interactions are fundamental for the development of the immune system. Drastic changes in modern environments and lifestyles have led to an imbalance of this evolutionarily ancient process, coinciding with a steep rise in immune-mediated diseases such as autoimmune, allergic and chronic inflammatory disorders. There is an urgent need to better understand these diseases in the context of mucosal and skin microbiota. This Review discusses the mechanisms of how the microbiota contributes to the predisposition, initiation and perpetuation of immune-mediated diseases in the context of a genetically prone host. It is timely owing to the wealth of new studies that recently contributed to this field, ranging from metagenomic studies in humans and mechanistic studies of host-microorganism interactions in gnotobiotic models and in vitro systems, to molecular mechanisms with broader implications across immune-mediated diseases. We focus on the general principles, such as breaches in immune tolerance and barriers, leading to the promotion of immune-mediated diseases by gut, oral and skin microbiota. Lastly, the therapeutic avenues that either target the microbiota, the barrier surfaces or the host immune system to restore tolerance and homeostasis will be explored.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [10] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [11] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [12] |
Ongoing climate change might, through rising temperatures, alter allergenic pollen biology across the northern hemisphere. We aimed to analyse trends in pollen seasonality and pollen load and to establish whether there are specific climate-related links to any observed changes.For this retrospective data analysis, we did an extensive search for global datasets with 20 years or more of airborne pollen data that consistently recorded pollen season indices (eg, duration and intensity). 17 locations across three continents with long-term (approximately 26 years on average) quantitative records of seasonal concentrations of multiple pollen (aeroallergen) taxa met the selection criteria. These datasets were analysed in the context of recent annual changes in maximum temperature (T) and minimum temperature (T) associated with anthropogenic climate change. Seasonal regressions (slopes) of variation in pollen load and pollen season duration over time were compared to T, cumulative degree day T, T, cumulative degree day T, and frost-free days among all 17 locations to ascertain significant correlations.12 (71%) of the 17 locations showed significant increases in seasonal cumulative pollen or annual pollen load. Similarly, 11 (65%) of the 17 locations showed a significant increase in pollen season duration over time, increasing, on average, 0·9 days per year. Across the northern hemisphere locations analysed, annual cumulative increases in T over time were significantly associated with percentage increases in seasonal pollen load (r=0·52, p=0·034) as were annual cumulative increases in T (r=0·61, p=0·010). Similar results were observed for pollen season duration, but only for cumulative degree days (higher than the freezing point [0°C or 32°F]) for T (r=0·53, p=0·030) and T (r=0·48, p=0·05). Additionally, temporal increases in frost-free days per year were significantly correlated with increases in both pollen load (r=0·62, p=0·008) and pollen season duration (r=0·68, p=0·003) when averaged for all 17 locations.Our findings reveal that the ongoing increase in temperature extremes (T and T) might already be contributing to extended seasonal duration and increased pollen load for multiple aeroallergenic pollen taxa in diverse locations across the northern hemisphere. This study, done across multiple continents, highlights an important link between ongoing global warming and public health-one that could be exacerbated as temperatures continue to increase.None.Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [13] |
The incidence of allergic diseases continues to rise. Cross-sectional and longitudinal studies have indicated that allergic diseases occur in a time-based order: from atopic dermatitis and food allergy in infancy to gradual development into allergic asthma and allergic rhinitis in childhood. This phenomenon is defined as the "atopic march". Some scholars have suggested that the atopic march does not progress completely in a temporal pattern with genetic and environmental factors. Also, the mechanisms underlying the atopic march are incompletely understood. Nevertheless, the concept of the atopic march provides a new perspective for the mechanistic research, prediction, prevention, and treatment of atopic diseases. Here, we review the epidemiology, related diseases, mechanistic studies, and treatment strategies for the atopic march.Copyright © 2020 Yang, Fu and Zhou.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [14] |
任华丽, 孙劲旅, 刘光辉. 过敏性疾病共病与多病的相关研究进展[J]. 中华预防医学杂志, 2022, 56(6): 735-739. DOI: 10.3760/cma.j.cn112150-20220312-00229.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [15] |
娄艳, 龚红辉, 曾立云, 等. 三级综合医院门诊多学科协作诊疗SWOT分析[J]. 中国医院管理, 2023, 43(5): 54-57.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [16] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [17] |
赵志雄, 龙入虹, 李萍, 等. 多学科诊疗门诊现状与质量控制——以广西某三甲医院为例[J]. 现代医院, 2024, 24(3): 402-405. DOI: 10.3696/j.issn.1671-332x.2024.03.020.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [18] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [19] |
Esophageal cancer is one of the most aggressive gastrointestinal cancers. This review focuses on eight topics within the multidisciplinary approach for esophageal cancer. As esophagectomy is highly invasive and likely to impair quality of life, the development of less invasive strategies is expected. Endoscopic resection (ER) of early esophageal cancer is a less invasive treatment for early esophageal cancer. A recent phase II trial revealed that combined ER and chemoradiotherapy (CRT) is efficacious as an esophagus-preserving treatment for cT1bN0 squamous cell carcinoma (SCC). Esophagectomy and definitive CRT are equally effective for patients with clinical stage I SCC in terms of long-term outcome. For locally advanced resectable cancers, multidisciplinary treatment strategies have been established through several clinical trials of neoadjuvant or perioperative treatment. Minimally invasive esophagectomy may improve the outcomes of patients and CRT is a curative-intent alternative to esophagectomy. CRT with 50.4 Gy radiotherapy combined with salvage surgery is a promising option to preserve the esophagus. Induction chemotherapy followed by esophagectomy may improve the outcomes of patients with locally advanced unresectable tumors. Immune checkpoint inhibitors are effective for esophageal cancer, and their introduction to clinical practice is awaited.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [20] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [21] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [22] |
The concept of multidisciplinary team discussion of patient's care has been a part of routine medical practice for several decades [Monson et al. in Bull Am Coll Surg 101:45-46, 2016; NHS. Improving outcomes in colorectal cancer-the manual. (Guidance on commissioning cancer services-improving outcomes). 1997.]. The idea of bringing multiple specialties and ancillary services together to help optimize patient outcomes has been implemented in several clinical arenas from burns to physical medicine and rehabilitation to oncology. In the oncology realm, multidisciplinary tumor boards (MDTs) originated as a broad-based meeting that would permit the review and discussion of cancer patients to optimize treatment strategies [Cancer Co. Optimal Resources for Cancer Care: 2020 Standards. Chicago, IL: 2019.]. Over time, as further specialization occurred and clinical treatment algorithms have become more complex, multidisciplinary tumor boards have become more disease site specific. In this article we will discuss the importance of MDTs, specifically focusing on rectal cancer MDTs including their impact on treatment planning as well as the unique interplay of clinical specialties that provide internal quality control and improvement. Additionally, we will discuss some of the potential benefits of MDTs beyond the direct impact on patient care and review some of the challenges of implementation.© 2023. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [23] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [24] |
张瑜洁, 王健, 曹硕, 等. 基于CiteSpace的多学科诊疗应用研究的热点与趋势分析[J]. 医学与社会, 2023, 36(7): 62-67. DOI: 10.13723/j.yxysh.2023.07.012.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [25] |
毛一晴. 基于政策工具的我国多学科诊疗模式政策内容研究[J]. 中国卫生事业管理, 2024, 41(1): 50-53, 83.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [26] |
GBD DISEASES AND INJURIES COLLABORATORS. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019[J]. Lancet, 2020, 396(10258): 1204-1222. DOI: 10.1016/S0140-6736(20)30925-9.
In an era of shifting global agendas and expanded emphasis on non-communicable diseases and injuries along with communicable diseases, sound evidence on trends by cause at the national level is essential. The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) provides a systematic scientific assessment of published, publicly available, and contributed data on incidence, prevalence, and mortality for a mutually exclusive and collectively exhaustive list of diseases and injuries.GBD estimates incidence, prevalence, mortality, years of life lost (YLLs), years lived with disability (YLDs), and disability-adjusted life-years (DALYs) due to 369 diseases and injuries, for two sexes, and for 204 countries and territories. Input data were extracted from censuses, household surveys, civil registration and vital statistics, disease registries, health service use, air pollution monitors, satellite imaging, disease notifications, and other sources. Cause-specific death rates and cause fractions were calculated using the Cause of Death Ensemble model and spatiotemporal Gaussian process regression. Cause-specific deaths were adjusted to match the total all-cause deaths calculated as part of the GBD population, fertility, and mortality estimates. Deaths were multiplied by standard life expectancy at each age to calculate YLLs. A Bayesian meta-regression modelling tool, DisMod-MR 2.1, was used to ensure consistency between incidence, prevalence, remission, excess mortality, and cause-specific mortality for most causes. Prevalence estimates were multiplied by disability weights for mutually exclusive sequelae of diseases and injuries to calculate YLDs. We considered results in the context of the Socio-demographic Index (SDI), a composite indicator of income per capita, years of schooling, and fertility rate in females younger than 25 years. Uncertainty intervals (UIs) were generated for every metric using the 25th and 975th ordered 1000 draw values of the posterior distribution.Global health has steadily improved over the past 30 years as measured by age-standardised DALY rates. After taking into account population growth and ageing, the absolute number of DALYs has remained stable. Since 2010, the pace of decline in global age-standardised DALY rates has accelerated in age groups younger than 50 years compared with the 1990-2010 time period, with the greatest annualised rate of decline occurring in the 0-9-year age group. Six infectious diseases were among the top ten causes of DALYs in children younger than 10 years in 2019: lower respiratory infections (ranked second), diarrhoeal diseases (third), malaria (fifth), meningitis (sixth), whooping cough (ninth), and sexually transmitted infections (which, in this age group, is fully accounted for by congenital syphilis; ranked tenth). In adolescents aged 10-24 years, three injury causes were among the top causes of DALYs: road injuries (ranked first), self-harm (third), and interpersonal violence (fifth). Five of the causes that were in the top ten for ages 10-24 years were also in the top ten in the 25-49-year age group: road injuries (ranked first), HIV/AIDS (second), low back pain (fourth), headache disorders (fifth), and depressive disorders (sixth). In 2019, ischaemic heart disease and stroke were the top-ranked causes of DALYs in both the 50-74-year and 75-years-and-older age groups. Since 1990, there has been a marked shift towards a greater proportion of burden due to YLDs from non-communicable diseases and injuries. In 2019, there were 11 countries where non-communicable disease and injury YLDs constituted more than half of all disease burden. Decreases in age-standardised DALY rates have accelerated over the past decade in countries at the lower end of the SDI range, while improvements have started to stagnate or even reverse in countries with higher SDI.As disability becomes an increasingly large component of disease burden and a larger component of health expenditure, greater research and development investment is needed to identify new, more effective intervention strategies. With a rapidly ageing global population, the demands on health services to deal with disabling outcomes, which increase with age, will require policy makers to anticipate these changes. The mix of universal and more geographically specific influences on health reinforces the need for regular reporting on population health in detail and by underlying cause to help decision makers to identify success stories of disease control to emulate, as well as opportunities to improve.Bill & Melinda Gates Foundation.Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [27] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [28] |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [29] |
纪和雨. 基于多学科诊疗的儿童过敏性疾病临床信息模型的研究[D]. 上海: 上海交通大学, 2020.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [30] |
李茜, 孙燕, 胡滨. 开展新形式门诊多学科联合诊疗模式的探索[J]. 中国医院管理, 2019, 39(1): 35-36.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [31] |
沈颖洁, 陈烨, 彭红, 等. 基于患者需求的多学科诊疗门诊精准预约运行分析[J]. 现代医院管理, 2024, 22(1): 42-45. DOI: 10.3969/j.issn.1672-4232.2024.01.011.
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| [32] |
王睆琳, 代佳灵, 梁蓝芋, 等. 线上线下融合的多学科诊疗服务模式实践[J]. 中国卫生质量管理, 2024, 31(2): 48-51. DOI: 10.13912/j.cnki.chqm.2024.31.2.12
{{custom_citation.content}}
{{custom_citation.annotation}}
|
| {{custom_ref.label}} |
{{custom_citation.content}}
{{custom_citation.annotation}}
|
/
| 〈 |
|
〉 |




{kind=link}